_square_md.jpg)
A population-level perspective on duration and care dynamics
Imagine two people, both aged 75, both living in a residential care home. On paper, they look identical to a population model: same age, same care state. But one arrived six months ago, following a fall. The other has been there for three years, her condition gradually progressing through earlier stages of disability before reaching this point.
Are they really the same?
Most models assume they are.
Any experienced care professional would say no. The person who has been in care for three years is likely to have less functional reserve, a greater comorbidity burden, and a higher risk of further decline. The duration of her stay is not just background information. It is a signal of how her condition is likely to evolve.
Yet when we model these dynamics at the population level, to project how many people will need care, what kind, and at what cost, duration typically disappears from the picture.
This is not because researchers have overlooked it. It is because the dominant tools have not made it easy to include.
A different way to model care dynamics
Most long-term care projections rely on microsimulation. This involves generating thousands of individual life histories under specified transition rates and averaging the results. While flexible, this approach can obscure the structural relationships between ageing, disease progression, and policy interventions. It becomes difficult to ask what role duration plays, or how much error we incur by ignoring it, when everything is embedded in simulated trajectories.
In recent work, I developed a deterministic alternative: a transport-based model that describes population flows directly, rather than simulating individuals one by one.
The framework builds on classical ideas from structured population modelling, where age-structured dynamics have long been studied. It extends these ideas to capture how long individuals have been in each care state.
There are two versions of the model.
The first tracks individuals by age only. People move between care states, healthy, mild disability, moderate disability, and residential care, at rates that depend on their age. This provides a transparent and mathematically tractable baseline.
The second adds a second clock: duration. In addition to age, the model tracks how long someone has been in their current state. Each transition resets this internal clock to zero, after which it increases as time passes. This turns a two-dimensional problem in time and age into a three-dimensional one: time, age, and duration.
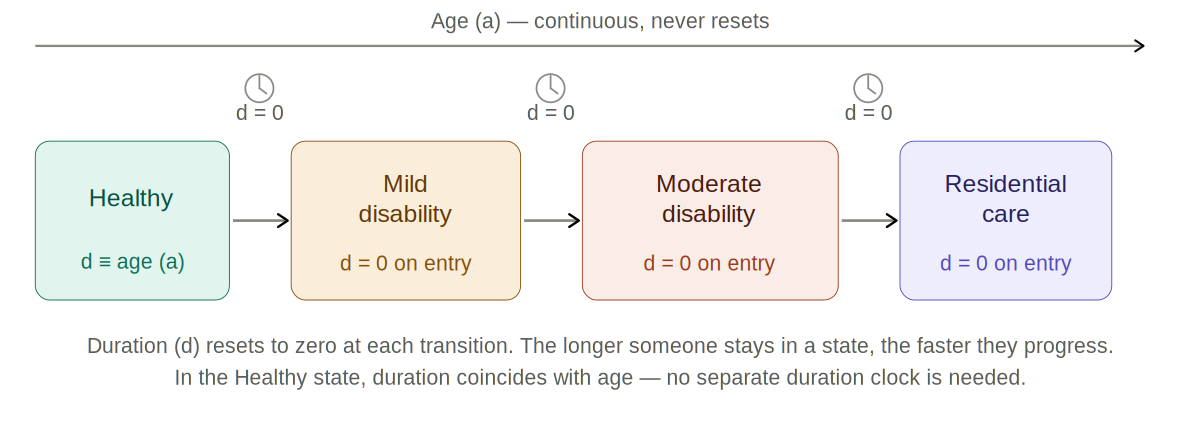
Figure 1. Care state transitions under the two-clock framework. Age advances continuously; the duration clock resets to zero at each transition. In the Healthy state, duration coincides with age.
When duration matters and when it doesn’t
The relationship between the two models is precise. If progression rates depend only on age, not on how long someone has been in their current state, then the two models give the same results. Integrating the duration-aware model over all durations collapses it back to the age-only version.
This is an important property. The richer model is a true extension, not a replacement. When duration is irrelevant, nothing is lost. But when progression does depend on duration, as clinical evidence strongly suggests, the two models diverge. And they diverge in a systematic way.
The hidden bias in standard models
Individuals who have spent longer in a disability state tend to deteriorate faster. Functional reserves decline, comorbidities accumulate, and disability progression accelerates. An age-only model cannot capture this. As a result, it retains too many individuals in earlier disability states and underestimates how many accumulate in advanced care states. This is not a random error. It is directional, and it grows over time.
Numerical experiments show that even moderate duration dependence leads to substantial differences in how the population is distributed across care states after twenty or thirty years. What makes this particularly important is that aggregate prevalence remains almost unchanged. The total number of people in non-healthy states looks similar in both models. But the internal distribution, which drives costs, is different.
When planning for long-term care, it is well known that residential care costs for complex needs are far more expensive than supporting someone with mild limitations at home. A model that underestimates advanced care states will therefore underestimate future costs, even while appearing to fit the overall prevalence well.
Why this matters for policy
The implications extend beyond cost projections. Consider a policy that reduces the rate at which healthy individuals develop disability, for example, through prevention or early intervention. In an age-only model, the effects are relatively straightforward. Fewer people enter disability states, and downstream impacts follow. In a duration-aware model, the outcome depends on the existing composition of the population. It depends on how long people have already spent in each care state (healthy, with mild limitations, moderately disabled, or in residential care) and how quickly they are progressing in each state. The same intervention might have amplified or dampened effects depending on this internal structure.
Ignoring duration can therefore lead to misplaced confidence in some policies and missed opportunities in others.
Transparency, not just complexity
One reason duration has often been omitted is due to computational considerations. Tracking duration explicitly increases model complexity. The framework, that I have recently developed, addresses this using a semi-Lagrangian approach, which follows individuals along their trajectories in age–duration space. This makes the model both stable and computationally tractable. More importantly, it makes the structure of the system explicit. Unlike microsimulation, which operates through large numbers of simulated life histories, the transport formulation describes population flows directly. The relationship between detailed dynamics and aggregate outcomes is transparent and mathematically exact. This makes it possible to identify, rather than assume, what drives long-term care demand.
Looking ahead
This work is primarily methodological. The current framework uses stylised transition rates rather than fully calibrated data. The next step is to estimate duration-dependent progression using longitudinal datasets, allowing the model to be applied directly to real populations. But the central point does not depend on calibration. If duration affects progression, and the evidence suggests it does, then models that ignore it will produce biased projections. The bias is systematic, it increases over time, and it is concentrated in the care states that matter most.
As populations age and long-term care systems come under increasing pressure, getting the structure of our models right is not optional. It is essential.
This blog draws on a forthcoming article: “A Semi-Lagrangian Framework for Age–Duration Structured Transport Models: Aggregation Consistency and Duration-Dependent Progression”by Mohamed Ismail. Details of the mathematical framework, numerical experiments, and aggregation consistency results are developed there in full.
About the author:
Mohamed Ismail is an Affiliate Research Fellow at the Oxford Institute of Population Ageing and Director of Analytical Research Ltd, working on mathematical models of ageing and long-term care dynamics.
Opinions of the blogger is their own and not endorsed by the Institute
Comments Welcome: We welcome your comments on this or any of the Institute's blog posts. Please feel free to email comments to be posted on your behalf to administrator@ageing.ox.ac.uk or use the Disqus facility linked below.
_square_xs.jpg)



_square_xs.jpg)





